Perifere vasculaire interventie
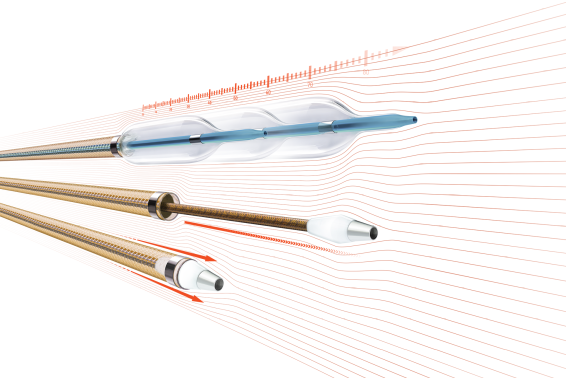
Perifere vasculaire interventie (PVI), ook wel perifere slagaderinterventie genoemd, omvat een verscheidenheid aan verschillende minimaal invasieve percutane procedures die worden gebruikt om een perifere arteriële aandoening (PAD) te behandelen. PAD is een aandoening waarbij de slagaders buiten het hart, meestal in de benen en voeten, vernauwd of geblokkeerd raken, meestal als gevolg van de ophoping van plaque. PVI heeft tot doel de bloedstroom in deze perifere arteriën te herstellen, de symptomen te verlichten en complicaties te voorkomen.